This weight reduction procedure is for the super obese patient, not everyone is suitable to have gastric bypass operation. This procedure is popular in the united states as the patients there generally have a higher BMI. The sleeve surgery is a more popular operation in Australia. Gastric bypass surgery is generally reserved for patient who have failed the sleeve surgery in Australia.
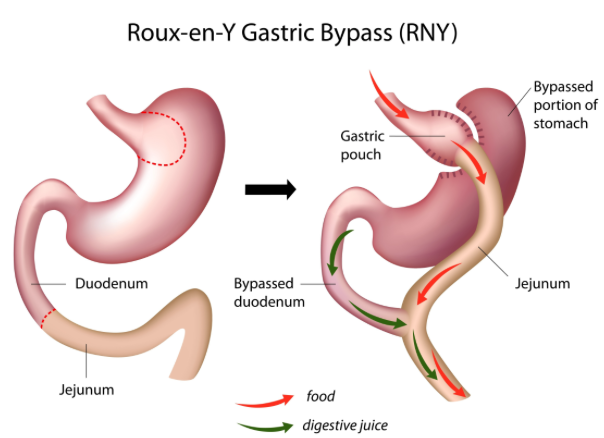
The Gastric Bypass takes advantage of both restriction and malabsorption to work. Consequently it is one of the most effective weight loss procedure. The entire procedure is performed laparoscopically. The average expected weight loss with the gastric bypass procedure is around 80% of excess weight in the first year. The weight loss is reduced to approximately 50 to 60% excess weight loss in 10 years. It is a complex procedure requiring formation of a small gastric pouch using stapling devices to divide the upper stomach and produce a 20-30cc pouch. The small intestine is divided about 75 cm from the point where it commences at the duodenum and is joined by stapling techniques to the bowel 150cm below the point of division.
Several forms of this procedure have been performed over the last three decades. It is based on an operation used to treat stomach ulcers and cancers for more than a century, and the name is derived from the name of the French surgeon who first described the use of a small segment of the small bowel to divert bile and acid away from the stomach and oesophagus. The current operation involves a restrictive element (considerably reducing the size of a part of the stomach) and a hormonal component (early passage of food into the intestine). These two factors give the strongest possible appetite suppression. This makes weight loss relatively straightforward in the great majority of people.
This operation has a very good combination of effectiveness (how much weight is lost) and durability (how long weight loss lasts). It avoids some of the dietary limitations of restrictive operations and the nutritional deficiencies of intestinal bypass operations. It accounts for 60 percent of obesity surgery worldwide.
Most of the published evidence leading to the worldwide acceptance of obesity surgery by government health agencies in Australia, the US, and the United Kingdom is based on gastric bypass surgery, which is the gold standard by which other weight loss methods are currently judged.
In some people, a ring can be placed around the stomach pouch during the operation to limit the risk of weight regain.
The effects of the surgery are:
- To reduce the amount of food the patient can eat.
- The opening from the pouch to the stoma is narrow, the food can only leave the stomach slowly, thus providing the patient with prolonged feelings of satiation.
- Sweet foods are not tolerated. The food the patient consumes enters the small bowel directly from the small stomach pouch. Eating sweet sugary foods produce a condition known as ‘dumping’. This is an unpleasant condition with feelings of sweating, anxiety, fast pulse and nausea.
- This deters patients from eating these fattening foods and thus aids weight reduction.
- Bypass may therefore be particularly suitable for patients who are addicted to sweets.
- Diabetes is often rapidly controlled due to the alteration in intestinal hormones. There is a variable length of small bowel bypassed producing a degree of malabsorption.
- This varies from 75cm to 150cm depending on how much malabsorption we wish to produce.
- The duodenum and upper small bowel is bypassed. This can produce nutrient malabsorption and deficiency. Iron and calcium deficiencies are common and protein deficiency can occur. Supplements must be taken to prevent the metabolic effects
Banded gastric bypass (Fobi procedure)
In larger patients or those who are habitual large–meal eaters, a ring can be placed around the gastric pouch to prevent softening due to forceful eating. Pouch softening may otherwise lead to increased capacity and later weight regain. Due to the ready availability of a high–quality band, the banded bypass is a routinely performed procedure, unless technical or patient factors make this unwise
Mini gastric bypass
This operation has been around for about 10 to 15 years and is becoming more popular, although not all outcomes are known. It has similar results to standard bypass but it is easier to perform (hence its increasing popularity). It has a lower risk of obstruction of the small bowel than a standard bypass, but higher risks of reflux. This may be the ideal operation for very overweight men for whom a standard gastric bypass may be difficult, or for patients with adhesions in the small bowel.
Questions and other information about Roux-En-Y Gastric Bypass
-
What are the benefits?
- More weight loss compared to the gastric sleeve or the gastric band
- Greater improvement in diabetes compared to the gastric sleeve or the band
- Suitable for revisional weight loss surgery
- Treatment for severe reflux
- Release of gut hormones promotes long term weight loss
-
What are the advantages of Roux-En-Y Gastric Bypass?
- The average excess weight loss after the gastric bypass procedure is generally higher in a compliant patient than with restrictive procedures.
- Studies show that after 10 to 14 years, patients on average have only gained back 10 to 13 percent of the lost weight.
- Significant sustained weight loss
- Blood sugar levels that become completely normal within 1 year of surgery
- Lower or normal blood pressure
- Lower or normal cholesterol levels
- Relief from sleep apnea, acid reflux and urinary stress incontinence
- Less arthritis pain and improved mobility
- Increased energy and ability to exercise
- Improved mood and self-esteem
- Arrested progression of heart disease
- Improvement of many lung conditions
- Exercise endurance
-
What are the complications?
The mortality rate for the procedure is approximately 1%. Anaesthetic complications, such as myocardial infarction and pneumonia, pulmonary emboli and wound infections can occur as with any procedure on the morbidly obese.
There is an incidence of complications of 5% to 10% specific to this procedure.
- Wound infections
- Reflux and diarrhoea
- Gastrojejunalstomal stricture
- Marginal ulcers
- Internal hernia
- Roux limb ischemia
- Blow-out of the stomach remnant
- Leak (The most serious problem that can occur, leakage from points where theintestine is joined together or to the stomach.) This can lead to infection and peritonitis and is the main cause of post-operative death.
- Small bowel obstruction can occur in the immediate post-operative period or later due to adhesions. ( this is less with keyhole surgery)
- Long-term micronutrient deficiencies (eg, vitamin B12, folate, iron, calcium deficiency with bone softening, anaemia and hypo-proteinemia).
Explore other weight loss & surgical procedures
Calculate your BMI
The Body Mass Index (BMI) is a measure for human body shape based on an individual's height and weight.
Contact us today to arrange a private consultation and discuss your options.
Book your appointmentServices
Locations
